Bridging the Gap – Fall 2015
Image
Reply


In health care, medical providers usually specialize in certain areas of expertise where they are at ease regarding anatomical systems, putative diagnostics, and technical vocabulary. Healthcare interpreters, on the contrary, are highly generalist on what comes to specialized terminology, and on top of that they have to be exceedingly fluent in more than one language. As anybody who works in this field might be aware of, in getting into the profession of medical/healthcare interpretation, interpreters walk into a complex path composed not of well signaled highways but of intricate networks with unending multiple sidetracked looping ramifications.
Besides being familiar with the patients’ background culture (especially in dealing with languages such as Arabic, French, and Spanish, due to the high cultural diversity of their speakers) it is also expected that while on duty, for the healthcare interpreter to be well versed on the culture of medicine at large (diseases, diagnostic tools, procedures, techniques, equipment, protocols, medications); something that implies the need for continuous learning mainly by new knowledge acquisition through reading, and by attending specialized courses and seminars.
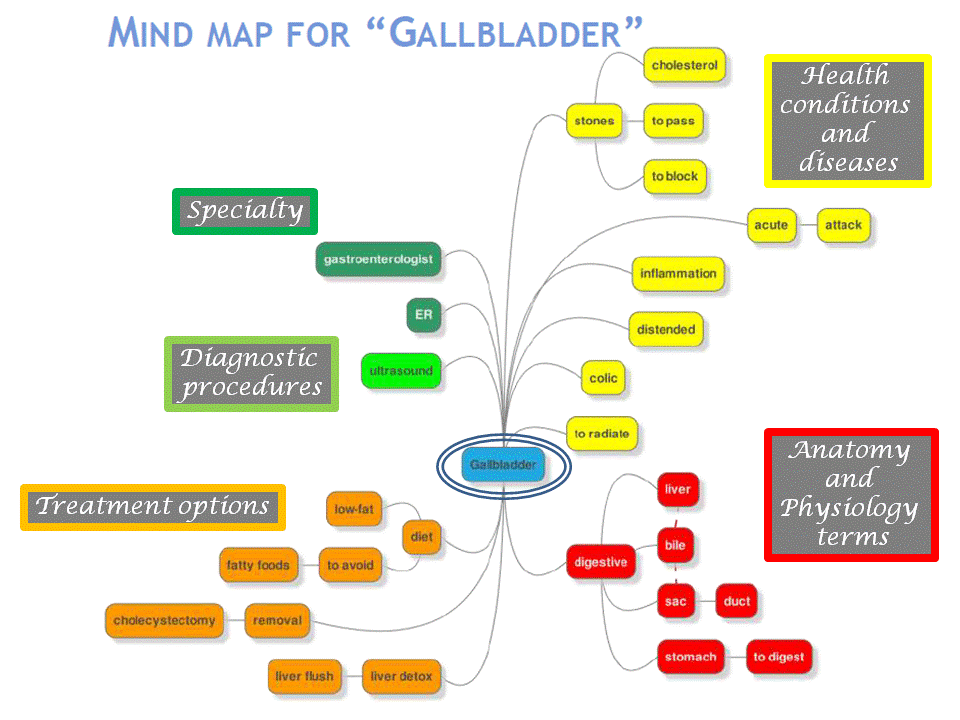
It was along those lines, and in order to help fellow interpreters get acquainted with useful techniques towards this goal that last winter, the CCHI Managing Director, Natalya Mytareva, presented within the CCHI’s online webinar series: Medical Terminology for Healthcare Interpreters: Disease, Disorders & Treatments of the Gallbladder. In there, using the gallbladder purposely as a mere example, she discussed some of the most up to date and innovative techniques developed with the background idea to help with vocabulary acquisition and terminology relationships.
Among those, mind mapping, although an ancient one, it has been proved a very useful technique in helping to relate ideas. Mind mapping mimics our brain’s ideas association patterns, and allow them to be portrayed as a diagram that uses a non-lineal graphical layout to construct intuitive frameworks around a central concept or subject.

Although a mind map may easily be drawn using pen and paper, software has been developed to such a goal and therefore, medical terminology relationships can effortlessly be established with the help of computerized frameworks, some of which can be accessed at:
There are multiple possibilities for building a mind map around a particular concept, putative branches, ramifications, and sub-ramifications that can be presented as a whole or in sections, depending on what is aimed at to be highlighted at a given stage of a particular study.
As an example of how a mind map can be constructed to help increase knowledge of a particular organ or system, and to provide awareness of the multiple relations that can be derived from it you can see here, out of several possible ones, a mind map built around the core of the gallbladder.
In regards to suitable ideas, techniques, and exercises for gaining vocabulary and building up terminology to improve interpretation agility, always paying attention to words and intention, healthcare interpreters can:
And to help with those self-training endeavors serve this short list of available resources as starting point for anybody interested:
Now that you have the tools you just need to find yourself some time to put them to practice. Enjoy!
